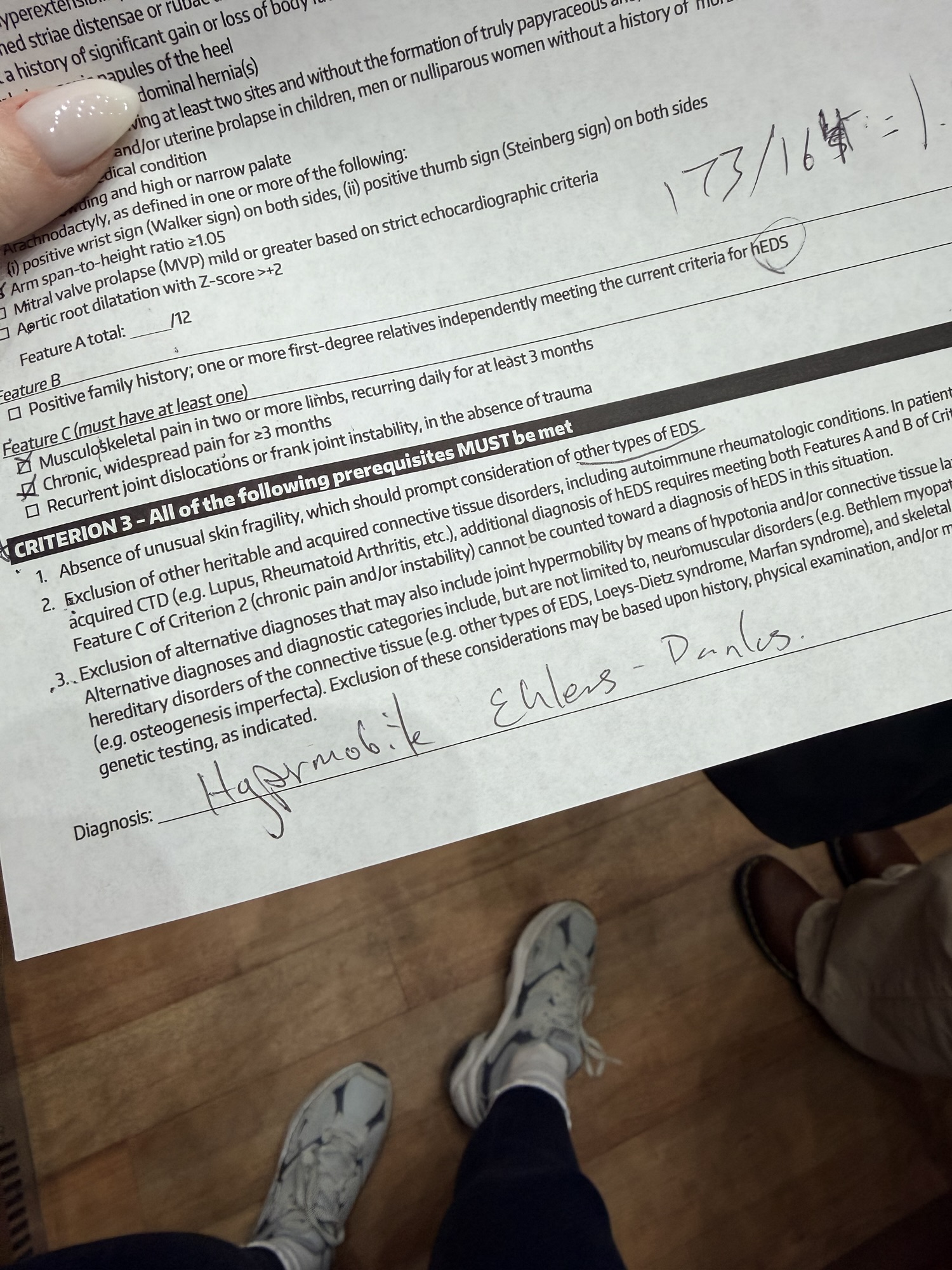
I was diagnosed with Hypermobile Ehlers-Danlos Syndrome (hEDS) last week. It been a very long journey. After eliminating autoimmune and other connective tissues disorders, I was referred to see a geneticist. There are 13 subtypes of EDS, with 12 of those having a verified genetic link to a specific gene. Unfortunately, the most common type, hEDS, has not yet found its associated gene.
So, after all my testing in bloodwork, ruling out the other rarer and sometimes life-threatening subtypes (such as Vascular or Cardio-Valvular), it was time for a clinical exam.
Unlike all the other forms, Hypermobile EDS relies on clinical criteria, patterns of symptoms, physical findings, family history, and systemic involvement. Medicine can only work with what currently exists in research, and research is still catching up. The criteria exists for a reason, as hEDS presents shared symptomatic patterns among the diagnosed. Yet without a confirmed gene, many still question the legitimacy or argue that the criteria needs further refinement.
The most well-known part of the evaluation is the Beighton Score, a 9-point scale used to measure joint instability. This looks for:
- Pinky fingers that bend back beyond 90 degrees
- Thumbs that touch the forearm
- Elbows that hyperextend past 10 degrees
- Knees that bend backward
- Palms that lie flat on the floor with straight legs
Points are added based on how many of these you meet. Joint instability isn’t the only issue, however. Full diagnostic criteria includes:
- Chronic musculoskeletal pain (I have a lot of stiffness and pain in those joints)
- Recurrent subluxations or dislocations
- Velvety and stretchy skin
- Atrophic scars, problems with healing, skin elasticity (hence why my stimulator “tore” off my spine twice and my incisions constantly opening)
- Hernias, organ prolapse, dental crowding
The Beighton Score still holds disproportionate weight in the conversation, which leaves parts of the evaluation outdated. Published in 2017, awareness exploded, research expanded, and the population being diagnosed began to shift in age, presentation, and complexity. Luckily, we now know more about comorbidities such as POTS and MCAS, the impact of gender bias, how flexibility can change, and the staggering number of patients that were dismissed for years before.
Someone who was extremely hypermobile at 15 (party tricks, anyone?), may not score the same as someone like me who is 34. Someone who has strengthened strategically may not look unstable in a five-minute exam. Someone (again, like me) with systemic involvement may not meet a strict numerical cutoff. Bodies change and age. Research advances. The process should too.
Luckily, in December of this year, there will be updated criteria to this evaluation (The EDS Clinic, 2026). This could include classification changes, diagnostic pathways, assessment updates, and treatment guidelines. The EDS community can’t predict the changes, but they do anticipate having more information on genetic markers, the Beighton Score, clarification of the hEDS and HSD split (Hypermobility Spectrum Disorders), and even subtypes of hypermobile EDS itself.
I feel like I am living in a gray area. Receiving a diagnosis like this means accepting complexity. The condition is real enough to disrupt daily life but not yet measurable enough to satisfy the skeptics. To me, hEDS explains everything from pain and stability issues to exhaustion and body-wide problems.
I will need to rearrange what my future looks like, and that can be scary. My care will shift from “trying things” to long-term management and it’s a pretty drastic shift. There is no cure for EDS, no medication that strengthens the connective tissue or stabilize joints, no surgery that fixes the underlying issue, and no option to heal with a snap of a finger. The only evidence-based way to slow progression and manage worsening symptoms is physical therapy. Strategic, stability-focused, controlled.
Typical exercise and working out will be different and it’s recommended that you don’t “push through” it. No medium- or high-impact cardio and strength training is a risky thing without proper therapy and guidance. Even water aerobics or resistance training must be supervised and progressed slowly. A few stretches of your hips and shoulders one day, knees and ankles the next. The more that is included in care, the likelihood of adding additional exercise can increase. Finding a specialized physical therapist is crucial and will essentially become the center of care.
Another piece is the role of mast cells. They influence inflammation, GI distress, systemic reactions, flares that seem disproportionate. Antihistamines will be a foundation while working with an immunologist who understands the overlap between EDS and dysregulation. Uncontrolled mast cells worsen everything.
My severity of Gastroparesis complicates it. EDS patients are statistically more prone to malnutrition, and its not due to intake, but rather impaired absorption. I will need a nutritionist who understands all my problems, particularly the interaction between EDS and Gastroparesis. The goal is not calories, but protein levels and accessible nutrients that don’t worsen the surrounding issues. Methods that bypass the traditional absorption pathways should be looked into, so I am not relying solely on a GI tract that is already severely compromised.
The relief in all of this is that with a clinical diagnosis, insurance and coverage shifts. Doors will open to accessible specialists and lifelong physical therapy. The layers of care I need and require will be more accessible.
The big things and the small things will also change. Standing in the kitchen, walking through a grocery store, typing at a desk, carrying laundry, sitting too long, traveling. All these things will go from simple tasks to becoming more difficult as my joints can worsen. Sitting is easier than standing and I will need to adjust my usual routine. Incorporating structured stretch breaks throughout the day and ensuring balanced movement will become a part of lifelong management.
This diagnosis does not end the life I hope to have, but it does reshape it. Moving slower and more consciously, often think about how to protect myself. There will be grief in that, which is not a new experience, but I have clarity, too. I understand the rules my body operates by. While I can’t cure any of this, I can choose to build a fulfilling life within it. It is still mine and I have so much to forward to.
Thanks for reading.